Health & Education
Trauma-informed care, medication-assisted treatment discussed at annual addiction medicine conference
By Danielle Harrison
Smoke Signals staff writer
The COVID-19 pandemic has left what are likely lasting scars and trauma for much of the population, be it through social isolation, job loss, a heightened sense of fear, illness or death.
For those with a substance use disorder, it also has resulted in much higher rates of overdose deaths and less access to in-person treatment, counseling or peer support groups.
A primary focus of this year’s American Society of Addiction Medicine annual conference was how clinicians can best assist those struggling with the added stressors of a global pandemic on top of managing a substance use disorder.
The society was founded in 1954 and is a professional organization representing more than 6,000 physicians, clinicians and other professionals in the field of addiction medicine. The organization’s goals are to increase access and improve the quality of addiction treatment, educate the public, and support research and prevention efforts.
The 52nd annual event was held in a virtual format for the second year in a row due to the pandemic.
In a keynote address on Thursday, April 22, society President Dr. Paul Earley referred to substance use disorders and COVID-19 as “intertwined epidemics.”
“In 2020, the overdose numbers got much worse” he said. “There was a 28.28 percent increase as of September. There has also been a significant rise in overdoses from multiple use of drugs. It’s rare to find people who overdose on one substance. There is also a much higher risk of getting infected with COVID if you have a past or present diagnosis of a substance use disorder, and you are more likely to suffer hospitalization and death.”
Earley cited statistics from a National Institute on Drug Abuse study involving the risk of hospitalization from COVID-19. Out of more than 12,000 patients who were diagnosed, hospitalization was 40 percent for whites with a substance use disorder and 50 percent for Blacks, compared with 30 percent overall.
“Drugs all target the cardiovascular system and interfere with immune responses,” Earley said. “These factors increase chances of being infected. Also, there are structural challenges, such as crowded methadone clinics at the start of the pandemic, and conditions in jail and prison systems. … One of the biggest problems is stigma. If people (with a substance use disorder) get infected, they are far less likely to go to an emergency room because of bad treatment in the past.”
Earley also discussed opportunities the pandemic had presented. For example, before COVID, most who visited methadone clinics could only receive their dosage in person, making it a challenge for those with small children, a job or lacking reliable transportation. Now, clients are allowed to have take-home doses, and those under quarantine could arrange for another person to pick up medication or have it delivered.
“The way that methadone delivery has changed is thought of positively by many clinicians and patients,” he said. “Other opportunities are the increased use of telehealth and changes in the justice system to allow the release of non-violent offenders with a substance use disorder from jails. However, despite these changes, it is harder to get patients into treatment during the pandemic.”
Earley also noted that much more marijuana and alcohol has been sold during the pandemic.
“Stress and uncertainty definitely plays a role,” he said. “The way people often deal with it is consumption of alcohol and drugs. With some, there may not be (long-term) negative effects, but with others it does. … We will be left with all of the devastation COVID has created. A lack of hope, helplessness, indifference and stigma all contribute to the devastating consequences of a substance use disorder and COVID.”
Numerous breakout sessions and workshops were held after the keynote address that touched on everything from medication-assisted treatment to the potential for safe injection sites with wraparound recovery services.
Stigma, anti-racism, compassion
and trauma-informed care
This session focused on addiction recovery and best practices to achieve success and was moderated by Dr. Vania Rudolf of Seattle’s Swedish Medical Center Addiction Recovery Services and Dr. Hendree Jones, executive director of the University of North Carolina’s Horizons drug treatment program.
Four women in recovery from a variety of racial and ethnic backgrounds spoke about the challenges they faced in finding substance abuse treatment and additional stigma that pregnant women and mothers deal with that are barriers to recovery.
The workshop also discussed how stigma-free, compassionate, anti-racist and trauma-informed care have potential to improve outcomes.
“Systemic racism doesn’t happen in a vacuum,” Jones said. “The war against substance use has been used to harm people of color.”
She cited President Richard Nixon’s domestic affairs advisor discussing the war on drugs to author Dan Baum. The adviser, John Ehrlichman, allegedly said that criminalizing possession of drugs like heroin and marijuana was intended to disrupt two of the biggest anti-establishment forces that opposed Nixon: Anti-war leftists and African-Americans.
There were common themes in the stories that the women in recovery told: Early exposure to drug use, being unaware of community resources, fear of being stigmatized, lack of housing, fear of having their children taken away, death of a loved one due to drugs and lack of wrap-around services for medication-assisted treatment.
“You get a prescription for suboxone and then it’s out the door,” one women said. “There needs to be more resources available. We want to be treated as human beings, ones who have made mistakes, and being given compassions helps.”
Evaluation and treatment of opioid use
disorders in remote areas with telemedicine
Anthony Dekker is an addiction and pain specialist at the Gallup Indian Medical Center in New Mexico. His areas of expertise include addiction medicine, chronic pain syndrome, high-risk youth, domestic violence and behavioral health. In the past, he served as chief clinical consultant in addiction medicine and chronic pain for the Indian Health Service.
The session focused on how the pandemic has brought many challenges to the evaluation and treatment of opioid use disorders and chronic pain syndrome, and how rural communities have experienced even more shortfalls.
However, the expansion of telemedicine has provided both opportunities and new challenges in the evaluation, treatment and documentation of opioid use disorder treatment, he notes, especially for veterans and Native Americans in remote areas.
“In 2020, the use of telehealth in opioid treatment was temporarily approved,” Dekker said. “It has allowed us to reach a lot more people in rural areas.”
He advised those doing virtual visits to have local public safety phone numbers handy in case a patient is in danger, getting consent for a virtual visit beforehand, knowing where the patient is calling from and if they have a private place to access reliable Internet service.
“Telemedicine has been a very important tool in treating opioid use disorder,” Dekker said. “Some patients also prefer telemedicine, especially in remote areas. It would be a step in the wrong direction if we lost our ability to use telemedicine.”
Best practices in managing
patients with kratom addiction
Cornel Stanciu is an assistant psychiatry professor at Dartmouth College and director of addiction services at New Hampshire Hospital.
An increasing number of Americans are turning to kratom for self-management of various pain, anxiety and mood states, and for those with opioid use disorders as an opioid substitute.
“People are using kratom to detox from opioids, to treat anxiety, pain and for relaxation,” Stanciu said.
Kratom is unregulated by the Drug Enforcement Administration and is sold at most convenience stores to anyone who wants it. Stanciu noted that kratom and morphine are very similar in their molecular structure, and kratom can lead to addictive behaviors over time.
After one year of regular kratom use, risks include lung injuries, high blood pressure, fatigue, constipation, seizures, hallucinations, elevated keratin levels, decreased liver function and, in some severe cases, kidney and liver failure.
“Most doctor’s offices don’t include kratom in routine screenings and most labs don’t know how to test for it,” he said. “When users stop, it’s a withdrawal similar to that of stopping opioid use. We don’t have a full understanding of it. Simple detox comes with a higher relapse rate, but there is no formal guidance on how to manage treatment. However, we have had success with medication-assisted treatments similar to those for opioid use disorder.”
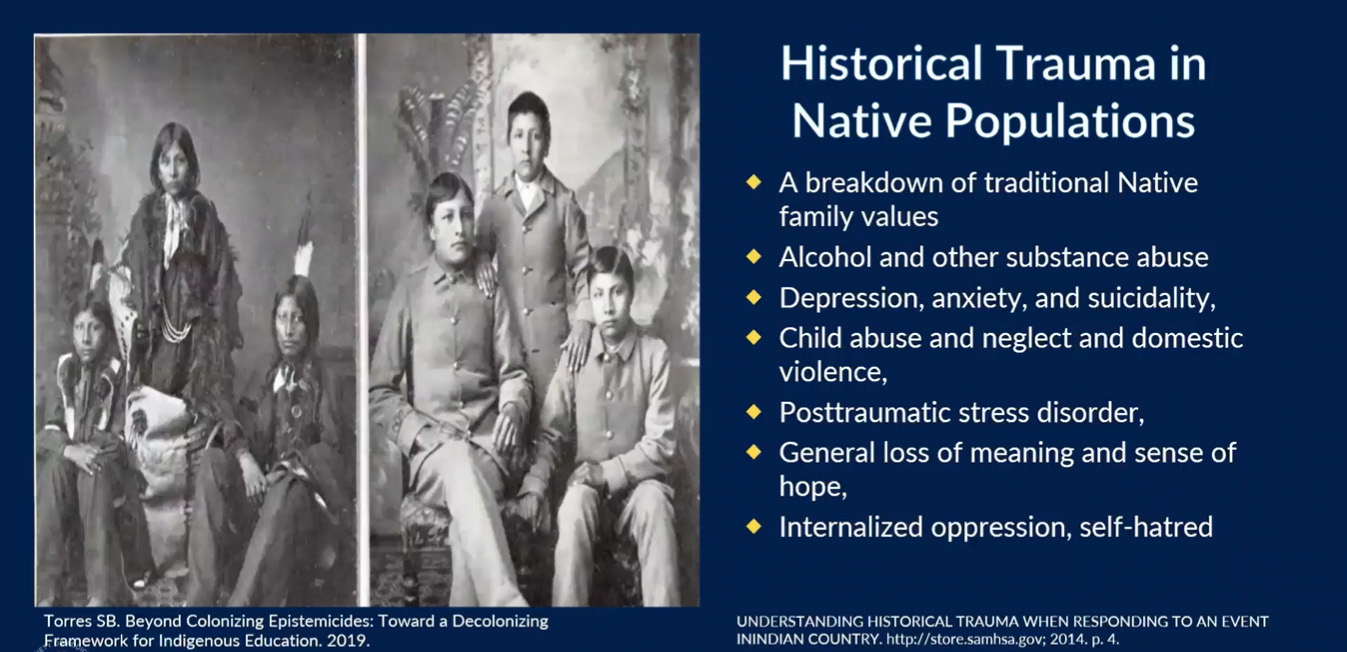
Neurobiology, historical and intergenerational
trauma and substance use disorders
Dr. Carolyn Ross, of Numinous Enterprises Inc. in California, discussed how ongoing research has documented the role that trauma plays in development of addictions, and how intergenerational trauma is also being explored in families of Holocaust survivors, African-Americans post-slavery and in Native Americans after violent colonialization.
Ross said that understanding the effects of trauma provides a more thorough understanding of addictions and other related disorders, and cites trauma as being an important underlying factor in addictions.
“Brain development is bottom up,” she said. “It begins with the survival center and ends with the executive center, which handles logic, reason and empathy. The brain has a lot of plasticity, but mostly at younger ages. What trauma ultimately can do is hijack a person’s potential in life. The problem begins even before birth, when a mother’s behavior has important effects on brain growth and development. Healthy attachment at birth makes it more likely a baby will have healthy relationships later in life.”
Additional factors, such as inadequate nutrition and toxic levels of stress in the first 1,000 days of life, can reverberate throughout a person’s life, Ross added.
“Trauma is the loss of an essential part of yourself, your safety, security, place and vitality,” she said. “It doesn’t change the DNA, but changes the expression of certain genes, and can take up to 20 years off a lifespan. The primary impact is to the brain. We can become hyper aroused or numbed out. We cannot reason ourselves out of being frightened or upset.”
She said the effects of intergenerational trauma can last through several generations.
“Kids are especially prone to the trauma in resettling in a new culture,” Ross said. “It can lead to depression, post-traumatic stress disorder and other conditions.”
Historical trauma includes five factors: Being deliberately inflicted on a target population, not limited to a single event, events reverberating throughout the community, the population being stripped of its culture and identity, and the trauma inflicted with malicious intent.
Both Native Americans and African-Americans were victims of historical trauma, which puts them at a higher risk of substance use disorder.
“It can also be very difficult to get treatment,” Ross said. “There are a lot of suspicions of the medical community and biases (toward patients).”